February 12, 2015
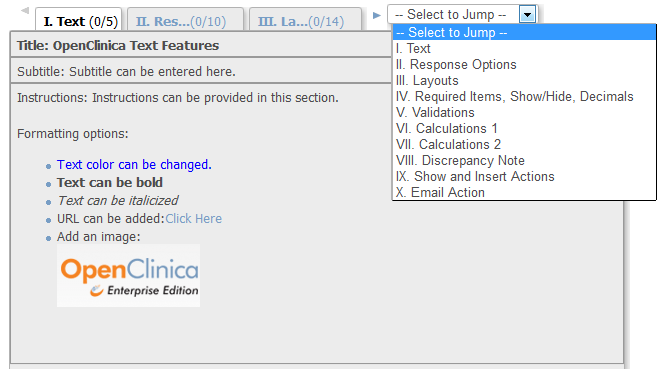
OpenClinica CRF Features – Everything But the Kitchen Sink
Whenever I teach case report form (CRF) design in the OpenClinica Central User Training class, the thought that always comes...
October 11, 2009
Rapid Deployment of New Functionality in OpenClinica Using MirthConnect
In a previous article, we describe how we at Geneuity Clinical Research Services exploit OpenClinica’s new web services feature to...
February 19, 2008
CDASH: A new way to standardize data elements
Many people who work with EDC systems have heard of or been impacted by CDISC, Clinical Data Interchange Standards Consortium. ...