February 12, 2015
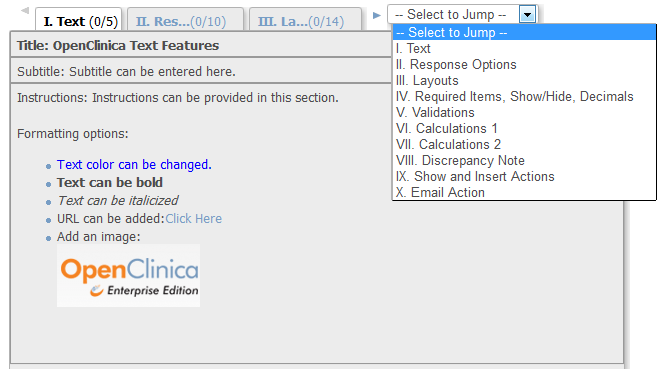
OpenClinica CRF Features – Everything But the Kitchen Sink
Whenever I teach case report form (CRF) design in the OpenClinica Central User Training class, the thought that always comes...
July 22, 2014
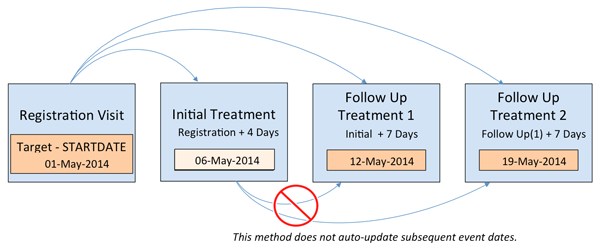
Automatic Event Scheduling with OpenClinica 3.3
An exciting new feature that has been at the top of the request list is Event Scheduling. Using the flexible...
August 3, 2011
eClinical Integration
Increasingly I am seeing real momentum for reducing the costs and barriers to integration of eclinical applications and data in...
June 13, 2011
OpenClinica 3.1 is Finally Here!
After nearly 20 months, OpenClinica 3.1 is finally ready to meet the world as a production ready application. It has...
October 26, 2010
New Capabilities Added to OpenClinica Version 3.1
For the past 12 months, the OpenClinica development team has been working diligently on the next major OpenClinica release. In...
July 29, 2008
OpenClinica 2.5 Release
We are getting very near to the release version 2.5 of OpenClinica, representing a major milestone in the development of...